It’s been way too long since I’ve written. I’ve been distracted by a number of concerns. But, I felt compelled to write about this sooner rather than later. No photos for this article. Just a quick and dirty composition of my thoughts on this incident.
You may have heard about the two dentists who were murdered in an altercation at their “Affordable Dentures & Implants” office in Tyler, Texas.
A disgruntled denture patient (of COURSE it was a DENTURE patient, RIGHT?) reportedly argued with the staff about getting a refund. He stormed out to his car and returned with a gun. He shot two dentists in the reception area. Both died.
That this is a needless tragedy and heinous crime is a forgone conclusion. Evil exists. Bad people exist. But, this hits home for those of us in the dental community. We’ve all dealt with difficult or angry patients.
Dentistry is a very personal service and business. The mouth and face are the most personal part of the body. Yeah… THE most… even more personal than the other place. Don’t believe me? Go touch a strange man’s butt and go touch a man’s face. One will start a fight. The other, perhaps an interesting conversation.
My point isn’t to be funny. But, I believe I’m right about a person who is already predisposed to anger may have his emotions boil over when he’s not happy with how things went in his mouth at a dental office. It’s as “personal” as it gets. I’ve written about violence at dental offices many times before on this blog. Sadly, it’s not uncommon.
I will try to be brief while turning this incident into a learning opportunity that may save lives in the future. This is a topic that should be discussed with your team. You have a plan for medical emergencies. Right? Do you have a plan for angry patients?
It should go without saying that DE-ESCALATION should always be the first resort. If a patient is angry or unhappy…. LISTEN first. Actually listen. Don’t talk. Listen. Let him get it out. Then ask what you can do to help. Then listen some more. Your staff should be alert to the situation and be ready to call 911 for help, if the signs of escalation are there.
The call to 911 should NOT be contingent upon the dentist asking for it out loud. In fact, if the dentist yells out, “Call 911,” it is likely to escalate the situation even more. Your staff should be trained to do it automatically (and quietly!) without your asking, when the signs are there. You also have a “benign” secret code word or phrase that triggers that call without alerting the bad guy to the plan.
What are the signs? Agitation. Yelling. Lots of arm movement. Shifting back and forth on his feet. Clenching fists. Touching his own face or hair repeatedly. Rapid blinking. Dilated pupils.
If any of that is observed, someone in the office should quietly make a call to 911.
If he storms out of the office, you should keep watching him. Did he get in his car and drive away? Or did he get in the car and sit there? Did he get back out of the car and start heading back to your office?? Have you called 911, yet?
You should LOCK THE DOOR immediately after he vacates the office. If he comes back and starts banging on the door… hopefully, you’ve already called the police. Step away from the locked door.
Situational awareness is the key here. Be aware of the signs. Try to de-escalate EARLY in the encounter. That’s the best case scenario. Keep your voice calm – no matter how raised his voice becomes.
If deescalation isn’t working, you need to put some distance / objects (like a counter or desk) between you and the agitated person. Do NOT initiate any physical engagement. Get away if at all possible.
If the disgruntled patient gets physical, defend yourself and your team. How you do that is way beyond the scope of this article. Hopefully, you can avoid it altogether. Ideally see it coming and deescalate or evade.
Edit to add (3/2/24) – It happened again:

 It turns out, this suicidal sociopath posted on Facebook that he wanted to “kill people and children.” It turns out, people that knew him, knew “something was wrong.” His ex-wife said he had been “acting strangely.” Nothing was said or done. Again.
It turns out, this suicidal sociopath posted on Facebook that he wanted to “kill people and children.” It turns out, people that knew him, knew “something was wrong.” His ex-wife said he had been “acting strangely.” Nothing was said or done. Again. 
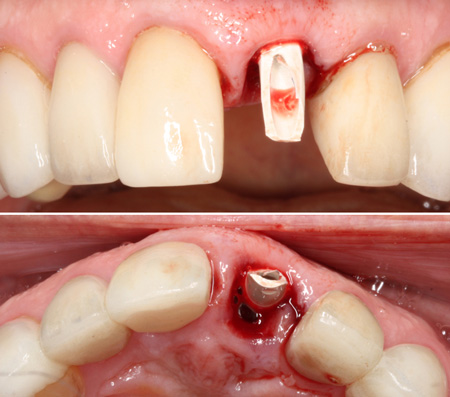
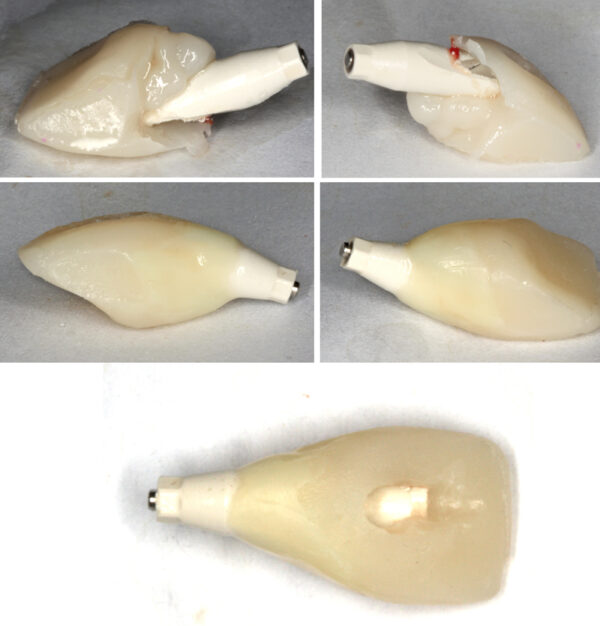
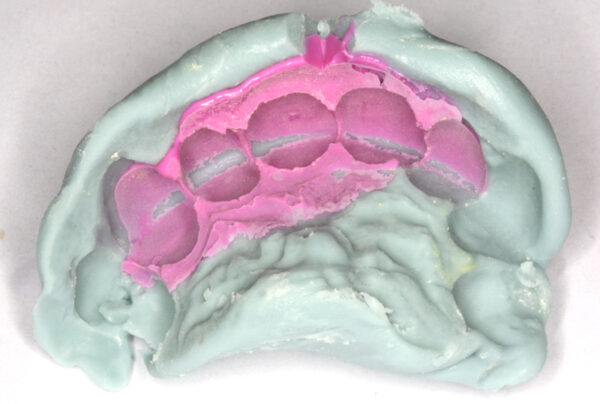
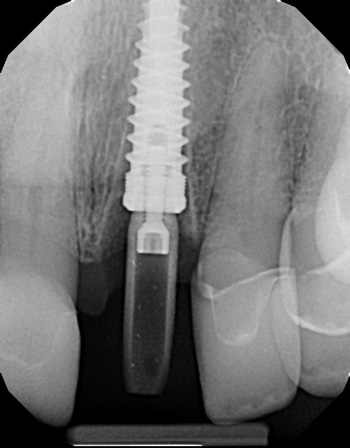
 While screw-retained implant crowns are favored today, certain clinical situations dictate cemented crowns on custom abutments. I won’t be going into the different scenarios that favor screw-retained over cemented. Nor will this article cover the advantages and disadvantages of each approach. I’ll assume you already know that… Or, you simply have your own preferences.
While screw-retained implant crowns are favored today, certain clinical situations dictate cemented crowns on custom abutments. I won’t be going into the different scenarios that favor screw-retained over cemented. Nor will this article cover the advantages and disadvantages of each approach. I’ll assume you already know that… Or, you simply have your own preferences. 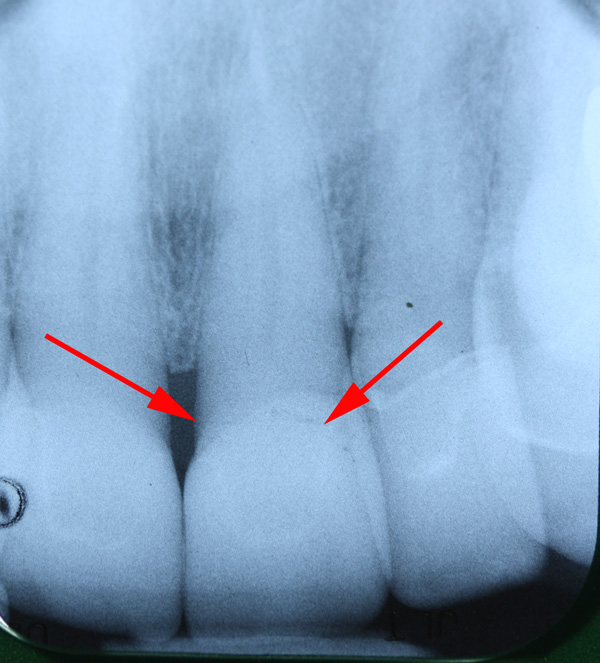


 Over the years, I’ve encountered colleagues that claim veneers are doomed to fail…. Or, that they are less predictable than crowns. “Veneers pop off.” “Veneers break,” they say.
Over the years, I’ve encountered colleagues that claim veneers are doomed to fail…. Or, that they are less predictable than crowns. “Veneers pop off.” “Veneers break,” they say.
 There are some serious potential problems with the COVID vaccines that are not being brought to light by those with the power to do so. The media and politicians are not discussing this at all. I’ve been reading the peer reviewed medical literature instead of listening to the talking heads. I have posted links and excerpts to three peer reviewed articles below. Decide for yourself.
There are some serious potential problems with the COVID vaccines that are not being brought to light by those with the power to do so. The media and politicians are not discussing this at all. I’ve been reading the peer reviewed medical literature instead of listening to the talking heads. I have posted links and excerpts to three peer reviewed articles below. Decide for yourself.