Over the years (since 1999), I’ve gradually added to my website. After 22 years, I’ve got over 50 pages on my site.

Something I’ve constantly advocated (to other dentists) is to avoid “catch-all” web pages on your website. For example: Putting a list of all your services on a single “Services” page dilutes the SEO (search engine optimization) potential for your website. Instead, put each service on its own web page.
If you offer veneers, for example, it deserves its own web page. If you put it on the same page as the laundry list of all your services, it simply won’t show up when someone searches “Veneers dentist my town.” A page dedicated to veneers is far more likely to get noticed (and more highly ranked) by Google. I’ve written about this before.

This time, it’s a bit different. This time it’s about the “About Us” page on your website. Most dentists have a “Meet the Dentist” page. Or (worse), they have a “Meet the Team” page that includes the dentist. The dentist should have his or her own page, of course. The team gets its own page, too.
Go tribal!
Typically on the “Meet the Dentist” page, we have the usual rundown of our qualifications and professional background, experience, and associations. BORING!!! Many will add something personal, as well… Like our family, pets, or our oil painting or fishing hobbies. BORING!
But, what if there was something about you that distinguishes you as different? Or as similar to a particular group of people? Continue reading →
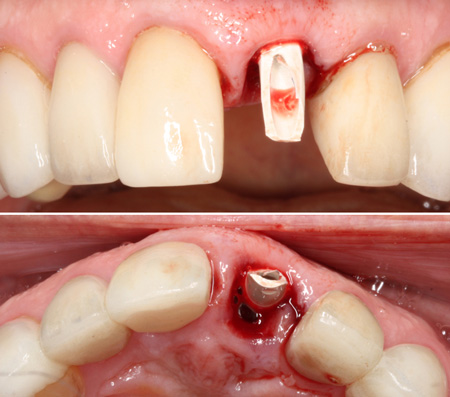

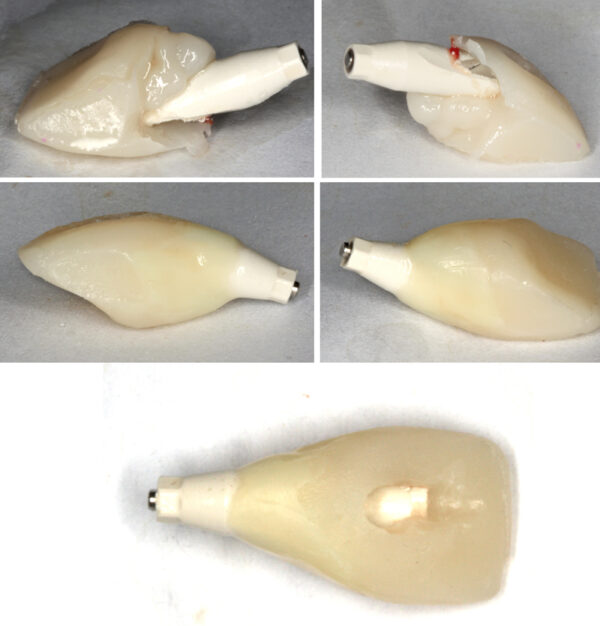
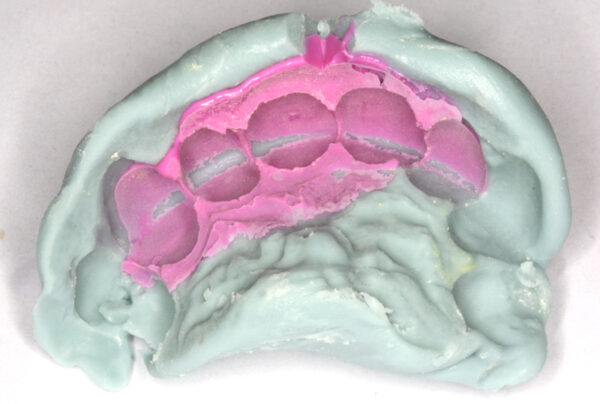
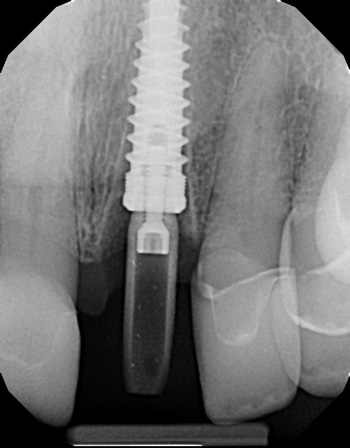
 While screw-retained implant crowns are favored today, certain clinical situations dictate cemented crowns on custom abutments. I won’t be going into the different scenarios that favor screw-retained over cemented. Nor will this article cover the advantages and disadvantages of each approach. I’ll assume you already know that… Or, you simply have your own preferences.
While screw-retained implant crowns are favored today, certain clinical situations dictate cemented crowns on custom abutments. I won’t be going into the different scenarios that favor screw-retained over cemented. Nor will this article cover the advantages and disadvantages of each approach. I’ll assume you already know that… Or, you simply have your own preferences. 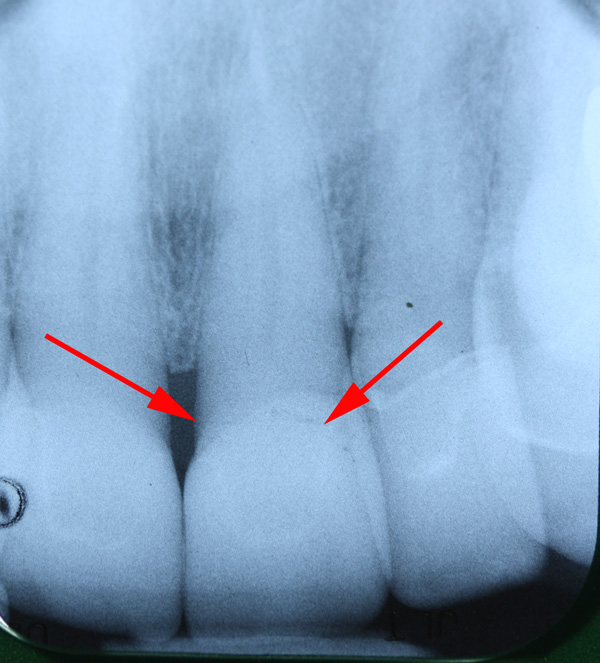
 Over the years, I’ve encountered colleagues that claim veneers are doomed to fail…. Or, that they are less predictable than crowns. “Veneers pop off.” “Veneers break,” they say.
Over the years, I’ve encountered colleagues that claim veneers are doomed to fail…. Or, that they are less predictable than crowns. “Veneers pop off.” “Veneers break,” they say.
 There are some serious potential problems with the COVID vaccines that are not being brought to light by those with the power to do so. The media and politicians are not discussing this at all. I’ve been reading the peer reviewed medical literature instead of listening to the talking heads. I have posted links and excerpts to three peer reviewed articles below. Decide for yourself.
There are some serious potential problems with the COVID vaccines that are not being brought to light by those with the power to do so. The media and politicians are not discussing this at all. I’ve been reading the peer reviewed medical literature instead of listening to the talking heads. I have posted links and excerpts to three peer reviewed articles below. Decide for yourself.

