Designs for Vision LED DayLite HDi Review
 I have previously written about the value of using magnification and a headlight. It’s a good time to revisit the idea, as I had to recently replace my headlight.
I have previously written about the value of using magnification and a headlight. It’s a good time to revisit the idea, as I had to recently replace my headlight.
I’ve been using my Designs for Vision “DayLite” along with magnification for many years. I think it has been at least 10 years that I’ve had the LED DayLite. It might be more. I’m not sure. I may call and ask the folks at DFV and come back and edit this article for accuracy. Before that, I went through several of the old fiber-optic lights.
Your mission, should you choose to accept it…
I use my DFV telescopes (they’re not actually “loupes,” though that is the popular term) with the headlight every single day… ALL day. They are what I call “mission-critical” equipment. They are as essential as my compressor and vacuum systems. I truly cannot operate without them. MISSION-CRITICAL. I would not try to treat patients without them, nor would I be a patient for a dentist who doesn’t use them. I really wouldn’t. So, yeah… call me a snob. I’m cool with that. 🙂
For several months, I’ve been having a problem with my old DayLite headlight. It was an electrical connection issue between the cable and the battery. So, the light would sometimes flicker on and off, depending on my movement. Even if I tightened the cable lock-nut down, it would intermittently cut off. If I loosened it, it would cut off. So, I’d have to fiddle with it to keep the light on, sometimes. It was frustrating to say the least. But, I hesitated to send it off for repairs, since I didn’t have a back-up. So, I just “dealt with it.”
Bohemia, we have a problem.

My old, now broken, DayLite.
But, then a couple of weeks ago, I noticed that where the cable connected to the headlamp unit, it was broken! Oh no! It was now connected only by the two wires inside the cable. This isn’t going to last long! And, I don’t want to be left hanging without a light! So, I called Designs for Vision (located in Bohemia, NY) and inquired about what to do. I could return it for repairs, of course. But, then I’m left with no light! Or…. I could get a new light… an even BETTER light.
I couldn’t really complain after beating on this light for 10 years or more.
I had already perused their latest product offerings on the DFV website. They have way more variety in their products today! I was intrigued by the new “cordless” headlights. The battery is self-contained in the headlamp unit that mounts on your glasses. The idea of not having a cable running down the temple of the glasses, back to a clip on the back of my collar, and then down to a battery pack on my belt or in my pocket was attractive.
Thankfully, I had a good discussion about how I use my DFV gear with my sales rep. Continue reading →
 Copyright protected by Digiprove © 2018 The Dental Warrior®
Copyright protected by Digiprove © 2018 The Dental Warrior®


 When it comes to the actual dentistry, many of us can be perfectionists and our own worst critics. I think that stems from the “beatings” we took in dental school. I remember being told to change the pulpal floor of my first Class 1 prep by a QUARTER-MILLIMETER. I thought the instructor was full of shit (well… most of them WERE!). But, now a quarter-millimeter is a “mile” in my eyes.
When it comes to the actual dentistry, many of us can be perfectionists and our own worst critics. I think that stems from the “beatings” we took in dental school. I remember being told to change the pulpal floor of my first Class 1 prep by a QUARTER-MILLIMETER. I thought the instructor was full of shit (well… most of them WERE!). But, now a quarter-millimeter is a “mile” in my eyes.


 It’s been a while since I’ve written! Busy with life and uninspired.
It’s been a while since I’ve written! Busy with life and uninspired.

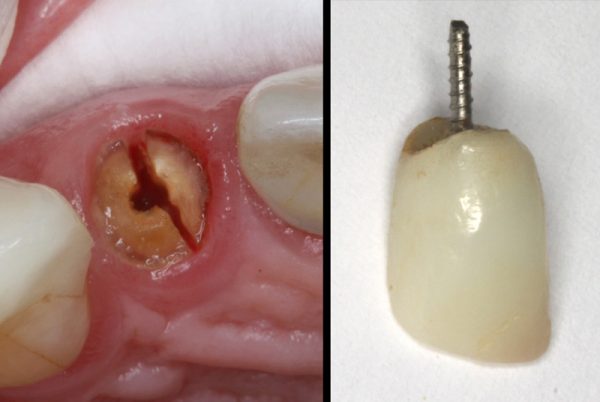
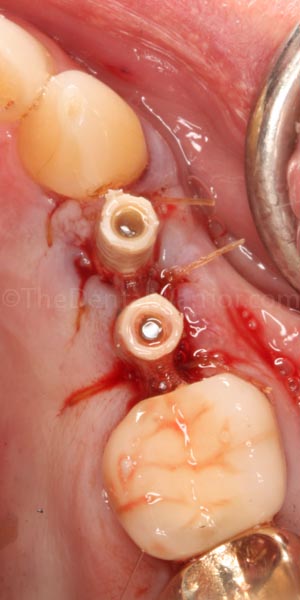
 Patient is a 90 y.o. male. He broke a big chunk of porcelain off a screw-retained 3-unit bridge, #19 – 21. The fracture was on #21, taking most of the facial and mesial porcelain off. This left what would be a big food trap on the mesial of #21, not to mention rather unsightly metal exposure in a semi-cosmetic area of the smile.
Patient is a 90 y.o. male. He broke a big chunk of porcelain off a screw-retained 3-unit bridge, #19 – 21. The fracture was on #21, taking most of the facial and mesial porcelain off. This left what would be a big food trap on the mesial of #21, not to mention rather unsightly metal exposure in a semi-cosmetic area of the smile.