It’s funny how things come in cycles / clusters. Immediate implant provisionals seem to be my “thing,” lately.
I enjoy the challenge, and each case is a bit different. So, it seems I’m inventing new techniques as I go with each case.
Today’s case is a new patient. She moved down, mid-treatment, from “up north.” Her periodontist up north had placed an implant in site #9. Apparently, #10 had been grafted to prepare for a future implant. In the mean time, she has been wearing an Essix retainer as a temporary.
Her periodontist up north referred her to a periodontist here, who happened to be “my periodontist.” And, then my perio referred her to me. The plan was for my perio, Dr. Gornstein, to uncover implant #9 and place implant #10. Then I would place immediate provisional crowns on both.
I started with an exam and study models. I sent the study model for a wax-up of #’s 9 and 10.

Patient presentation pre-operatively. She also requested replacement of crown #11.
Instead of getting a wax-up back, I got what appears to be a printed model and a putty matrix (I didn’t request the matrix – usually make’em myself, but OK).

Not bad… but, #9 and 10 are longish. I can correct intra-orally.

Putty matrix from lab.
The appointments were set, and the patient would come directly to my office from the perio.
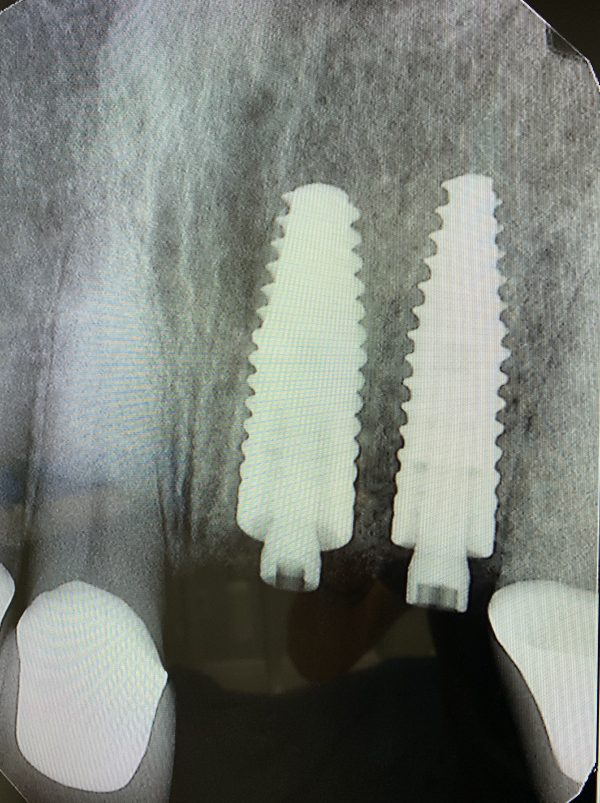
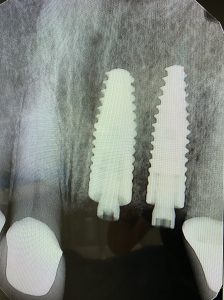
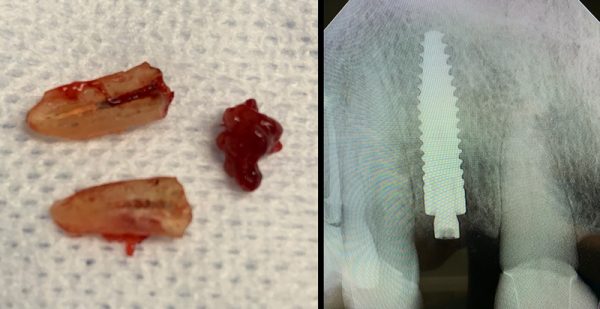
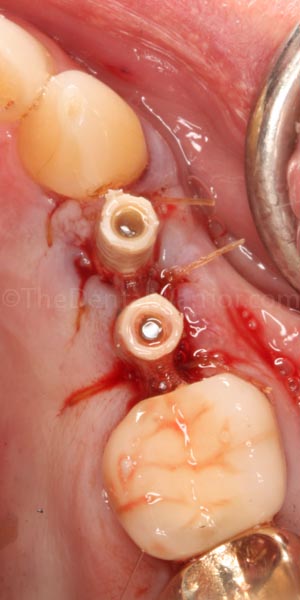
Implant #10 added by my local periodontist.

This is how the patient presented at my office immediately post-surgery. The periodontist provided the “PEEK” temporary abutments.
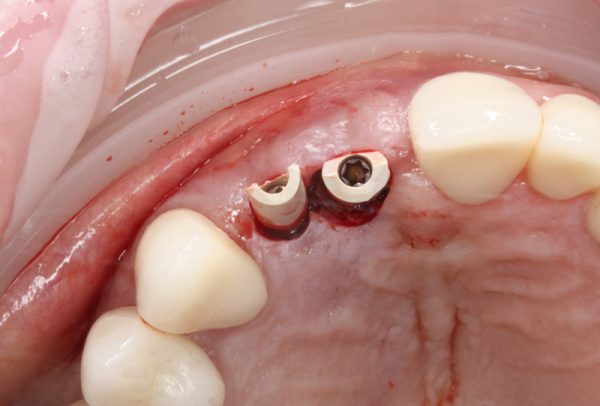
Occlusal view immediately post-surgery.
As I initially examined the surgical result, I didn’t think I’d need to reduce the temp (PEEK) abutments, but I wasn’t sure. The putty matrix is opaque, so with that, I could only “feel” if there was any interference. But, I wouldn’t be able to see if there was adequate clearance to avoid “show-through” of the abutments in the provisionals.
Then it occurred to me Continue reading
 Copyright protected by Digiprove © 2019-2020 The Dental Warrior®
Copyright protected by Digiprove © 2019-2020 The Dental Warrior® 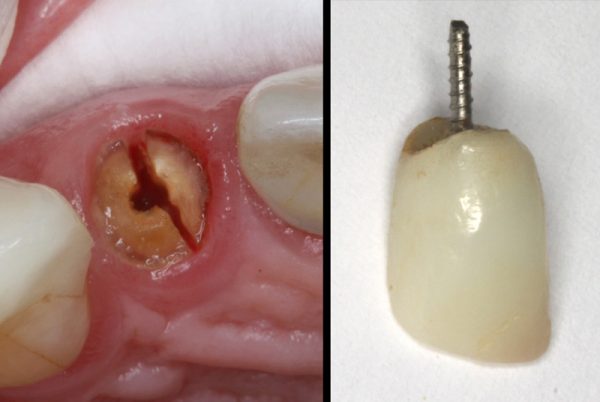


 When it comes to the actual dentistry, many of us can be perfectionists and our own worst critics. I think that stems from the “beatings” we took in dental school. I remember being told to change the pulpal floor of my first Class 1 prep by a QUARTER-MILLIMETER. I thought the instructor was full of shit (well… most of them WERE!). But, now a quarter-millimeter is a “mile” in my eyes.
When it comes to the actual dentistry, many of us can be perfectionists and our own worst critics. I think that stems from the “beatings” we took in dental school. I remember being told to change the pulpal floor of my first Class 1 prep by a QUARTER-MILLIMETER. I thought the instructor was full of shit (well… most of them WERE!). But, now a quarter-millimeter is a “mile” in my eyes.


 It’s been a while since I’ve written! Busy with life and uninspired.
It’s been a while since I’ve written! Busy with life and uninspired.

 Patient is a 90 y.o. male. He broke a big chunk of porcelain off a screw-retained 3-unit bridge, #19 – 21. The fracture was on #21, taking most of the facial and mesial porcelain off. This left what would be a big food trap on the mesial of #21, not to mention rather unsightly metal exposure in a semi-cosmetic area of the smile.
Patient is a 90 y.o. male. He broke a big chunk of porcelain off a screw-retained 3-unit bridge, #19 – 21. The fracture was on #21, taking most of the facial and mesial porcelain off. This left what would be a big food trap on the mesial of #21, not to mention rather unsightly metal exposure in a semi-cosmetic area of the smile. I have previously written about the value of using
I have previously written about the value of using 