
Some days, I feel like I’m the dental version of a fireman. On Monday, I saw a new patient who had been referred to me by a colleague in Ohio (who knows me through the Dentaltown message boards). The patient is a “snow bird” who spends his winters in Florida. It happens a lot, as it seems there is a rule that most patients up North eventually end up in Florida. I share many patients with my northern colleagues.
First Fire
The patient, a 75 y.o. male with a history of multiple myeloma, had a chief complaint of a loose bridge. It was implant-supported with abutments in the position of #9 and #13. Interestingly, rather than pontics, there were crowns on natural teeth in the positions of #10 and #11. There is a pontic #12. So, it was combining natural teeth and implants. Except, the natural teeth were no longer really part of the equation (as you’ll see below)
The patient was planning to return home to Ohio in a couple of weeks. Normally, I’d recommend replacing the screws with new screws (and I told him so). The old screws have been stressed cyclically and are prone to breakage. But, he wanted a quick fix, and I thought I’d just tighten the existing screws enough to get him home to Ohio. And, so that’s what I did. I recommended that he see his dentist ASAP when he gets home. I also mentioned that the entire bridge may need replacement.
He’s baaaaack
Yesterday, the patient called to tell us the bridge came out completely. Rut-roh! I knew the screws did not likely loosen themselves all the way out in a couple of days. And, I was right. Both screws broke off in the implants. Oh, crap. I saw him this morning, and this is what I found.

Here’s what was under the bridge.

Two sides of the bridge.

X-ray of #9 – 10
#13 – screw was pretty close to the surface.
So, now what? OK… let’s see if we can get those screws out. I explained to the patient that it may not be possible, in which case, we could make him a temporary partial denture. If I could get them out, I would contact someone at 3i Biomet (a big implant company that is nearby) to see about getting replacement screws. But, first I need to try to remove the broken screws. I rescheduled my next patient (a crown delivery) and worked through part of lunch.
The first screw (#13) was closer to the surface, so I went for that one first. I was able to use an explorer and back it out in small steps. Hooray! My confidence was up.
Reality check! Not so easy!
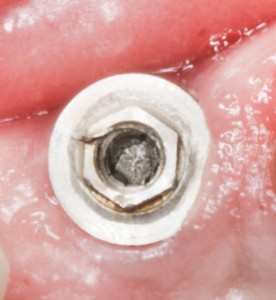
#9 – screw was deeper down inside the implant body. Do you see that little “bleb” in the metal at about 10 o’clock on the hex? I noticed that in the photo. When I went back the next day to deliver the new screws, I checked it out. It was a sliver from the top of the implant body threading that had stripped off. And, it would have prevented complete seating of the bridge abutment. I was able to grab it with a hemostat and peel it off.
Then, I tried the same approach with #9, which was deeper inside the implant body. I could see it barely moving, but it wasn’t rotating. So, I VERY carefully attempted to cut a little slot in the top of the screw without boogering up the implant’s internal threads. Then I modified a screw driver’s blade to a smaller size. It moved! A little. And, then it didn’t. Back to the handpiece. And, then the screw driver again. It took me at least an hour to get it out. But, I got it! It was a good feeling. The patient said, “You worked your butt off to get those out!”
I called my contact at 3i Biomet and sent him an email with the same photos you see here (and a few more). I sent the patient home and told him that we’d give him a call as soon as we got any news. In a couple of hours, I was told they had the screws, and at the end of the day, I drove about 30 minutes north to their headquarters and picked up the screws. I’ll be seeing the patient tomorrow morning on my day off. (I’ll update this article after I see him tomorrow.)
Update on Fire #1
I saw the patient this morning – by myself, as the office is normally closed on Fridays. I was relieved to see that I had the right screws (they fit). It was obvious that the ONLY thing holding this bridge in place was the screws. The bridge is destined for failure. But, we pressed on. The patient is in town only a few more weeks, and then he’s heading home to Ohio. I urged him to see his dentist there ASAP. While the patient is concerned about extracting the two roots because of his diminished ability to heal (multiple myeloma), I explained that the teeth could become a source of infection.

The screw in #13 was nearly flush with the surface of the broken porcelain. There was room interocclusally for me to add some composite. You can see the teflon tape under the composite.

A problem I noticed was that the wrench shaft was binding on the facial side of the screw hole access. As a result, the wrench was not fully seating into the hex of the screw. And, that would prevent proper tightening (and torquing) of the screw. So, I widened the access hole with a diamond, which allowed the wrench to be used without binding and align / seat fully in the hex…. or to borrow from the Endo world – “straight line access.”
I checked the occlusion, and made some adjustments to take some of the load off.
The patient was happy with the result, as was I!
Fire #2
This was a new patient coming in for a consultation / 2nd opinion. He was a 20 y.o. who came with his mother. They found me via a web search. And, they drove SIXTY MILES to see me! There are probably a few hundred dentists between their home town and my location.
His chief complaint was that he had a crown done recently (1 week ago) that he didn’t like. The tooth had been previously restored with “bonding” multiple times. He stated that the new crown felt big, and there was a sharp spot on the back. The patient mentioned that the crown was done in a day with a “scanner.” Mom said she didn’t know that he’d be getting the crown the same day, so she wasn’t there to approve the esthetics. He came home with it cemented in place. Upon examination, I could see that it was a veneer (or 3/4 crown).

Front view of the CAD/CAM restoration #8.
Apparently, there was a small diastema between #8 and #9, which was closed with the CAD/CAM veneer. From this front view, it doesn’t look so hot, but I’ve seen worse.

Side view of #8.
The patient’s biggest complaint is that it “feels big.” Let’s look at it from another angle:

Hoo-boy! Tooth #8 appears to be in her third trimester!
Mom, patient, and I looked at these same photos on the iPad. Mom asked if I could just “take it down.” Patient explained his biggest fear was that if he went back to the treating dentist, and he wanted to re-do it, that there would be no tooth left to restore. He read it on the internet. I explained that the veneer could be removed without further reducing the tooth underneath. Not a problem at all. I also explained to Mom that most dentists, myself included, would not want to reshape the veneer placed by another dentist. I described that it likely had surface stains that, once “sanded down” would cause a color change.
The wheels on the bus…
I explained that some dentists would insist on restoring BOTH central incisors, because it would be easier to match. I said, “Your dentist was conservative on two levels. First, he didn’t insist on restoring the other incisor just to make it easier. He attempted what we know as the most difficult cosmetic procedure, which is to do just the one tooth. And, sometimes we don’t get it perfect on the first try. Secondly, he did a veneer instead of a crown. He saved a lot of the good natural tooth structure.”
I recommended that he return to the treating dentist and give him a chance to make it right. I re-emphasized that the patient need not worry about his tooth being reduced to “nothing.” Both he and his mother were VERY relieved and thanked me profusely. They said that if they couldn’t get it resolved, they would return to my practice. I smiled and said, “I’m here if you need me, but I bet you’ll get fixed up with no problem.”
So there’s a dentist in a town 60 miles north of me that will never know who saved him from an oncoming bus. It is a good feeling!
So, those were today’s fires. What say you? Comment below!
 Copyright protected by Digiprove © 2015 The Dental Warrior®
Copyright protected by Digiprove © 2015 The Dental Warrior®
Great writeup, love your pics and captions (almost lost it on the “trimester”).
We all experience this and most of us try to go the extra mile for our patient’s and our own satisfaction. The real question is how did you charge for the first fire? It’s easier with these if they don’t have insurance…
No insurance involvement. Heck… what would be the “code?” Is there such a thing?
Good job, Mike. You get to wear your cape and shiny boots today. 🙂 Keep up informed about #1….fascinating case! It’s those cases that force you to think outside the box that make dentistry exciting.
Put him back together this morning. The new screws worked. But, they are the ONLY thing holding the bridge in place. I adjusted the occlusion a bit, too.
I’m on a little “vacation” at the moment. So, I’ll see about posting updated photos.
Really cool of you to allow the previous dentist to rectify the situation. We’ve all done work that’s not our best effort on a particular day. It’s a tough call because they have their doubts about the previous Dr (with good reason) and obviously trust you, and you know you can definitely do a better job.
Unfortunately, neither of these patients had any chance of being happy with the work that was placed. Many of the failures that we treat and see were destined to be failures on the day that they were inserted. Dentists always act surprised when things fail; the real surprise is that anyone could think that they could succeed.
Yep. But, when playing fireman, you can only do what you can do… within the parameters that have already been set and within the abilities, resources, and availability of the patient. Ideal treatment is not always possible… at least at a given moment in time. Maybe later.
Hi Mike;
I would agree with you 1000% IF these things happened once in a great while and finances were a significant burden. The young man PAID for a crown that was below the standard of anyone’s standards and the 75 year probably paid a hefty sum for his bridge.
These failures are failures of diagnosis or treatment planning and not bad luck or ‘cheap’ dentistry.
Ah… I thought you were referring to the implant case, primarily. That was what I was mainly talking about in my previous reply.
The 75 y.o. probably did pay a hefty sum for his bridge…. 15+ years ago. I paid a hefty sum for my 2004 Subaru STi. In fact, I bet I paid more for my Suby than he did his bridge. 🙂 I put 192,000 miles on it, including hundreds of laps on the track at triple-digit speeds. I drove the shit out of that car, and I had a BIG GRIN the whole time. I replaced the engine once. And, that engine finally gave up several months ago. The car lasted “only” 11 years, which is considerably less than this guy’s bridge. Should I complain to the dealer that sold me the car? 😉 Should I write a nasty letter to Subaru? Should I go on social media and tell all my friends that Subaru makes crappy cars?
As for the single central incisor veneer case… Yeah, I would agree it’s below the standard of most dentists. I could use it as an opportunity to bash CAD/CAM dentistry. I’m NOT a fan of what I see as representative of CAD/CAM. But, that would be like blaming a set of golf clubs for a bad game. Every dentist can have a bad day. The real measure of the dentist will be how he remedies the situation, eh? I’m afraid many dentists would have thrown him under the bus without giving him a chance to fix it. What would you have done, Gerald?
Hi Mike
Interesting points!
Re the bridge: Both the patient and the dentist got lucky. The restoration lasted longer than it probably should have since the natural teeth didn’t have much of a feral.
Re the crown: No comment
The other point that your blog addresses is do we have a ‘responsibility’ to fix everything that walks into our offices since much of it, like the above bridge were ‘end game’ the day that they were placed? (End game meaning that those teeth could not endure any additional treatment).
When patients present for a consult and give me any indications that they have to, need to, want to place ANY limitations on treatment options, I just tell them that I don’t have the skills needed to fix their problem. I can’t fix the unfixable and I can’t fix stupid so why try to be a hero, get behind schedule and lose money in the process.
Always enjoy your blog.
gerald
These are so difficult I have had people that come to me and want a new crown and you give them the option of more crowns so that they all match. The problem is they still go with just the one crown. Then they are unhappy. Most of the time you have to recall to the patient that you gave them both options. But what about the ones that never come back to you to explain that this was their decision. Anyway, doesn’t happen often with me just thinking of how this all happens.
I love your blog. I wish my blog to be like yours one day.
Thanks, Richard. I have heard that some dentists will insist on doing BOTH central incisors, just so they will match (more easily). I have not done that and just can’t bring myself to cut down the other tooth just to make it easier.
This is not a tough shade matching case. I would perform though a composite restoration on left central so the 8 won’t be so wide.
I enjoy so much your blog. Cheers!
Yep. I agree. I would either keep the diastema or do some bonding to add to the mesial of #9 and “meet in the middle.”
Hey Dental Warrior can I ask what you use for your comments in wordpress…. if you don’t mind.
I’m just using whatever came with the theme, I guess. I’m using iThemes “twenty-ten” theme.
Thanks. You are awesome
Great post. My youngest daughter said ewwww to number #8. I am sure that I have done worse on a bad day. It appears that #7 would benefit from some bonding on the mesial then #8 could be made to more appropriately fit #9. I do a lot of single centrals. Everyone one of which I swear will be my last…but I press on….I wouldn’t want my perfectly fine tooth cut down either. Some play with the m and d- facial line angles would also help.
Great fix with the implant/tooth bridge. My Irish lass is asking why does that girl (boy) not have any teeth? Ahhh to be a preschooler. I digress. teeth and implants do not belong together. PDL movement versus implant osteointegration = bad. But they did not know this for awhile. 3i is just great, I love that company. I have no idea how that screw could have been torqued in without proper access. A lot of time I seat the screwdriver then attach the handle to the latch attachment…just to be sure…but again, I have my days to0. I have also found that an explorer and patience works well. Apparently there is also a tool 3i makes called an “easy out”. I am not sure how it works but an OMFS I refer to has one. The only thing worse than a screw breaking is the implant breaking. My father has seen only a few of these in 20+ years of implant dentistry. I cannot imagine how awful it must be for the patient to get this out.
Thank you as always for your informative posts with humorous twists! Happy St. Paddy’s Day!
Thanks for your insightful comments, Elle! I recently heard about that tool from 3i. I haven’t looked into it, though.
I enjoyed your blog. Composite restoration would be more conservative than doing veneer to close the diastema.
Interesting pics here. It’s great to see you working through patient’s problems despite the difficulties. Keep up the good work!
Picture tells a thousand word at a time and you prove it again. in both cases you just simple impress me. I like your advise to the patient in Fire#2 case and recommend another chance to rectify the dentist the situation.
I just become a fan of this blog. A special thank to The Dental Warrior for sharing such a nice post.
Good for you Mike! I appreciate what you did for the dentist of the 20-year-old patient. That was very professional and it made me proud that we work in the same profession. On the other hand, dentists should ensure they’re doing the right thing and remember it is our responsibility to make our patients happy and healthy at the end of the day. Dentists might be surprised when they get it wrong, but they’ve got to fix it.
Thanks. But, I can’t help noticing that apparently “Matt” from Linteau Consulting is posting comments on behalf of Dr. Preston. 🙁
If you’re going to be active on social media, the doctor should be doing it herself. “Just sayin’.” 🙂
I often wonder if the dentists that hire these guys know what they’re doing (and not doing), to justify billing them. Basically, you’re paying them to spam blogs.
How do I know that’s the case here? Because the person posting the comment has a different email (and a different name) and a different location (ip) than the dentist’s website in the link. That, and the comment doesn’t sound like a dentist’s way of talking. 🙂