
Well, since my entire day’s schedule cancelled due to a tropical storm and tornado warnings…. I’ve got time to post this case.
Long time patient. Very nice guy. Has some pretty severe wear on his anterior teeth. Got him wearing a night guard every night.
I have bonded fractured incisal edges on his upper centrals a few times for him. Even with a night guard, he keeps losing them.
We decided to crown the central incisors. I advised him of the potential for endo.
I took a pre-op impression and waxed things up, and adjusted the opposing model to test how much interocclusal space I might be able to gain.
Got him in to prep. Managed to avoid endo… I think… for now. I borrowed from Peter to pay Paul when it comes to occlusal clearance. I hope it’s enough.

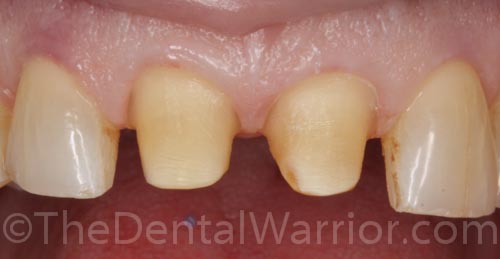
Pre-op

Pre-op: I can see my pulp from here!

Oy! Can we fit crowns in there? Without doing a full mouth rehab?
Prepped! Magnification and a good headlight sure help!
I don’t normally like the preps this tapered. But, by the time I did facial and lingual reduction, the incisal third of the preps were pretty thin and sharp. So, when I round-off / smooth up the sharp corners, I end up with a more tapered prep.

Preps.

I think we can. I think we can. I recontoured the lower anteriors to gain some interocclusal clearance. Side benefit of recontouring lowers… Patient noticed they were smoother!

Custom stained temps.

Temps.

Impression.

Impression porn! I didn’t use retraction cord. I didn’t use the laser.

Same view with flash on one side only to show texture. Impregum rocks.
 Copyright protected by Digiprove © 2013 The Dental Warrior®
Copyright protected by Digiprove © 2013 The Dental Warrior®
What material did/are you going to use. I had a similar case 7-8-9-10 worn down and you could see the pulp. I used all zirconia crowns because I had so little lingual clearance. The case turned out pretty good. He had a mosaic of different colored teeth showing. It was a compromise on getting a color. But he was happy.
http://thepasadenatexasdentist.com/index.php/blog-5/cosmetic-dentistry-solutions/
Hi Michael,
I’m thinking either Emax or PFZ (zirconia). But, PFM with metal occlusion is an option, too.
Your linky no worky! 🙂
weird, I click the link an it pulls up just fine. I liked the zirconia crowns as the lingual were so thin. I was freaking scared to even prep anything on the lingual with the teeth so already worn. Emax doesn’t do good thin right?
Hmmm… I tried again and no go.
“Firefox can’t find the server at http://www.thepasadenatexasdentist.com.”
double G.V Black strange, I am using firefox and both links go straight to my website. I sent one of my dirtbike buddies a link to a blog article I wrote on my http://www.shootingdentist.com website and he could not open the link either. Strange things are afoot at the circle k. (Bill and Teds Excellent Adventure reference) That is no good people can’t find my website. I guess I should check my Dentist Ultimate Guide to Website Version Two book!!!! 🙂
Something isn’t right. I searched for your site on Google, and it’s showing up. But, if I click the link (from Google), I’m still getting the not found error.
Hi Mike;
The treatment that you performed is very nice and well done. The problem is that your diagnosis and treatment planning was incomplete.
Diagnosis: 1. anterior teeth in the zone of function contributing to significant wear. The
cuspids are palatally inclined and the incisors are inside the cuspids.
2. teeth in zone of function in the presence of gastric reflux
3. Irregular mandibular anterior teeth
Treatment planning:
1.move the incisal edges labially either restoratively or orthodontically
2. eliminate the gastric reflux
3. orthodontically move the mandibular anterior…recontouring may or may
provide long term results.
Using a stronger material like Zirconia will only cause the next weak link to fail ie fractured tooth as the incisal edge position has been restored to its original (failed) position.
The beauty is: time will tell
Hi Gerald!
Actually, we already know about his parafunctional and GI issues. The patient is simply not interested in ortho and full mouth rehab. However, I DID get him to accept an occlusal guard, and he actually WEARS it every night. It took me years to get him to THAT point. 🙂 Don’t assume the diagnosis was incomplete, just because the treatment is “incomplete” in the eyes of a dentist. Patients don’t always accept what WE feel is ideal. We do what we can sometimes.
If I recall, patient is in his 70s.
He was in temps for a good while, and they survived.
Also… I did some significant recontouring of the lower incisors. Even the patient remarked, “Much smoother!”
So far, so good. 😀
Hi Mike;
My main concern is that we let our patients control the treatment plan which violates biology, laws of physics (2 things cannot occupy the same place at the same time) or DNA, we, the dentist assume all of the responsibility for an outcome that will eventually fail. The night guard is great but most of that damage occurred in function and not parafunction. We sometimes agree to perform treatment that we should beg off on.
As I said, the beauty of everything that dentists place is that we WILL know the eventuality of the case. 🙂
Trust me…I hope that he passes away before you have to find out. loll
How do you assert that the damage happened in FUNCTION? To my knowledge and experience, teeth actually don’t TOUCH in normal function. From my 25 years of experience and 2,000++ hours of C.E., that damage is from PARAFUNCTION with some GERD as “gas on the fire.” So, I totally disagree with your position on the etiology of the wear.
I have 100% confidence these restorations will hold up very well. This ain’t my first rodeo.
I also disagree with your characterization of “the patient controlling the treatment plan.” Honestly, that’s an insult. But, in a sense, the patient DOES have control… as it should be. Perhaps your practice style is dictatorial and paternalistic. Mine is a cooperative and educational effort rather than confrontational. I listen to my patients’ chief complaints. And, then I offer options. Rarely is it an all-or-nothing proposition.
Got some time to look back on old posts. To quote a certain President, you were…. WRONG. 🙂 Except the hedge of “time will tell.” Time DID tell.
The patient is still in my practice. We did this case seven years ago, and nary a problem. He wears his night guard religiously. No fractures. Not even a tiny chip. 😛
I completely agree with how you handled the case. Our job as dentists are to present and explain all of the options and the pros/cons of each. The patient gets to make the final decision on their treatment; therefore they should “control the treatment.” Very few patients, if any, are going to accept full ortho in their 70’s.
I also look at the patient’s previous history of broken porcelain or teeth. If there is none, we know all the wear has come from the acid reflux and the crowns should have a very long lifespan.
Thanks for your comments, Jonathan.
I’ve seen the patient a few times since treatment. So far, so good. He wears his night guard religiously.
Almost two years later, and these restorations are intact without any issues whatsoever. 😀
I’ll have to try to remember to take some photos next time he’s in for a recall visit.
To repeat the nested comment to Gerald… Patient still in my practice…. crowns 100% intact…. SEVEN YEARS later. 😛