 I love what I do for a number of reasons. I like the combination of engineering, biology, physics, and art that goes into restoring teeth and smiles. I like that we can eliminate a patient’s pain, usually in a single visit. And, I like that our efforts can literally change lives for the better.
I love what I do for a number of reasons. I like the combination of engineering, biology, physics, and art that goes into restoring teeth and smiles. I like that we can eliminate a patient’s pain, usually in a single visit. And, I like that our efforts can literally change lives for the better.
I’m always touched when a patient takes the TIME to go that “extra mile” in showing his or her appreciation for what we do. They pay us for our services, of course. And, that should be enough, right? But, some patients are compelled to go further and thank us in a number of ways. Sometimes it’s baked goods. Sometimes it’s a hug. Sometimes it’s a nice card. And, sometimes they even take the time to write their heart-felt thoughts. I got this card and letter this week:
Dr. Mike, Jo-Ann, Sandy, and Marcy,
 I woke up this morning thinking about how blessed we were to have found your office. I was thinking about how stressful it was worrying about Mary and all of her dental issues before she became a patient of yours.
I woke up this morning thinking about how blessed we were to have found your office. I was thinking about how stressful it was worrying about Mary and all of her dental issues before she became a patient of yours.
Finding your office was truly a blessing. If we had stayed at her previous dentist office, I don’t know if I would have survived the continual problems and stress that came along with having a dentist that didn’t want to hear or understand what I wanted for my beautiful daughter.
Every person in your office has played a crucial role in creating the beautiful, perfect smile that my daughter is so very proud of. It makes my heart so happy seeing what a difference your entire team has made in our lives.
Dr. Mike, I especially want to thank you for being so patient with me. I wanted certain things a certain way, and you never once questioned me. You went above and beyond to make it happen, and happen it did! Against all odds, Mary’s Maryland bridge is as solid as ever. I don’t know that you will ever fully understand what an impact you have had on our lives, nor could I ever thank you enough.
Forever grateful, The Smiths.
This family has gone out of their way to thank us before. Before I remade her Maryland Bridge, I did some bonding. I blogged about it previously. Here is a sequence of photos demonstrating the new Maryland bridge:
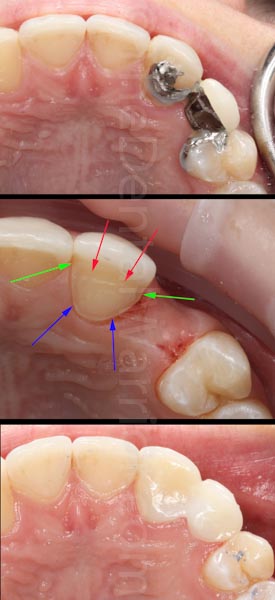
The old Maryland Bridge had debonded multiple times, and it was unesthetic. I decided to make the new MB as a cantilever to eliminate the potential for debonding on one side, which is common with bilateral abutments. I prepped the “lateral incisor” (really a canine) with a chamfer (blue arrows), vertical grooves (green arrows), and a horizontal groove (red arrows). The final MB is porcelain fused to a zirconia framework.
What can we learn from her letter? Patients want a doctor who LISTENS. It has taken me years to learn to do that, and I’m still learning. Many of us (myself very much included) are quick to interject our “expert” opinion at every opportunity. Learning to “shut up” is a valuable skill! And, in this case, I listened to both the mom and my patient, her 13 y.o. daughter. When I did speak, I made sure to address the daughter, as well.
A note like this from a patient really provides perspective and makes all the effort worthwhile. To borrow from Mel Brooks’ “History of the World”…. It’s good to be the dentist.
Update 2/4/21: There were some folks (see comments below) that felt this was inappropriate treatment… it wouldn’t last. The patient was in my office earlier this week. The cantilevered Zirconia Maryland Bridge is still there. It has not debonded once, in nearly 6 years. Hopefully, I have not jinxed myself by writing this!
Update 3/18/25: I saw this young lady for a hygiene recall today. This cantilever Maryland Bridge is still going strong at 10 years! It’s never debonded, either. Not once.
Awesome.
Reply
Great Job, Dr. Mike !
I am new to your website and blog and find it incredibly inspirational to read such articles from you.
I’ve been out of school for 9 years now and finally decided to stop working full time for a dead end corporate job, and started my practice 6 months ago from scratch.
Although new and struggling, I have faith and keep pushing on against the odds, and it fills me with confidence to know that I think along the same lines as you, and if that be the case, I must win..eventually..but surely !
Thanks again.
Reply
Hi Ritesh. Thanks for visiting my blog and taking time to post a comment! Good luck with your new practice!
Reply
Mike: I have seen a lot of nice work from you in the past…which leaves me even more, puzzled and shocked over your treatment plan for this case!
In spite of what you show with all your arrows: I can’t make out the retentive grooves beyond a bit of imagination ala “Emperor is Wearing Clothes”).
And, why a cantilever, (in the CANINE area!!!).
What “listening to the patient” convinced you to do it this way?
Reply
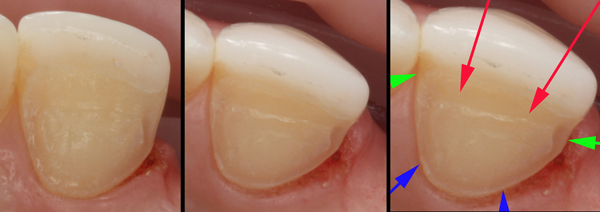
Hi Michael! The prep is very minimal / small, and the photo doesn’t show them very well. I’ll see if I can enhance the photo. But, the grooves are there, I promise! 🙂 The retainer actually had retention without cement, due to the prep.
The abutment is her actual canine. Mom wanted minimal prep. Mom was a former dental assistant, BTW. I didn’t see any advantage in involving the premolar. The premolar was involved with the first MB, and it kept debonding (and later, the retainer BROKE). I spoke with my lab about the design of the bridge, which was entirely my idea, incidentally.
The patient is 14 y.o. She did NOT want a “flipper.” She’s not a candidate for an implant, yet. This was deemed a compromise treatment from the “git-go,” and it was discussed as such with Mom. I told her I wasn’t sure how well it would work.
It’s been 9 months since I placed the new MB. So far, so good! I’m betting this will work quite well for quite some time. And, that’s what we’re doing… buying time.
Here are the best images I’ve got:
Reply
It’s now been four years. It has not de-bonded even once, yet. 😀
Reply
Patient was in last week for hygiene. She’s now 24 years old. So we’re at almost exactly 10 years of longevity. It still looks good and has not debonded even once.
Still shocked at this case? 🙂
Reply
Great case Mike as usual. I’d like to ask you a somewhat related question with cases like these or with cases in general small or big, how do you handle premature fee questions? (And I guess for that matter questions about the cost in general?)
Reply
Hi Ken,
I’m not sure I understand the question in the context of this case. If a patient asks for a fee for a big case “prematurely” (before I’ve formulated the treatment plan options), I simply tell them that I need to sit down and plan the case before I can answer it accurately.
Reply
Sorry Mike, my question really doesn’t pertain to this case specifically but in the future I’d like to see you do a piece on properly handling fee discussions for larger cases.
Reply
Ah… OK. I’ll put that on the list. In the mean time, did you see this?
Treatment Plan Presentation – Big vs. Small
Reply
Awesome job! I am betting on your cantilever. Maryland bridges don’t like to go around curves. They work well in a straight line but when flexure occurs in two different angles you get debonding (think vector physics). e.g. 23-24-25 works well if relatively straight. 22-23-24, not so much if teeth follow the natural curvature of most arches. It was very smart to have it just bonded on the one side and then cantilevering it.
Great post and the Aspen Dental post was spot on…it is just sad. I don’t understand how people can be taken in by that stuff. Didn’t their parents every tell them that nothing is ever free?? Just like my “free CE course” this fall….all I had to do was join a 2K a year study club. LOL. Hope my free course is worth it, so far the study club has been very useful.
Reply
Thanks, Elle. Time will tell with the cantilevered MB. But, it just made sense to me. I’ve always liked Albert Einstein’s quote that applies to many things in life: “The definition of insanity is doing the same thing over and expecting a different result.”
Reply
Dentists absolutely need to listen to their patients. After all, our role is to help make them smile! If we neglect to listen to their needs, they’ll leave our office feeling stress, not happiness.
Reply